
[Free Full Texts] Foramen magnum growth in achondroplasia
What is the central nervous system (CNS)?
The nervous system has two parts: the central nervous system and the peripheral nervous system, due to their location in the body. The central nervous system (CNS) includes the nerves in the brain and spinal cord. It is safely contained within the skull and vertebral canal of the spine. All of the other nerves in the body are part of the peripheral nervous system (PNS). Pubmed Health
The central nervous system consists of two parts: the brain and the spinal cord.
The brain works like a central computer. It processes information that it receives from the senses and body, and sends messages back to the body. Brain tissue is made up of about 100 billion nerve cells (called neurons) and one trillion supporting cells which stabilize the tissue.
The spinal cord is the highway for communication between the body and the brain. When the spinal cord is injured, the exchange of information between the brain and other parts of the body is disrupted.
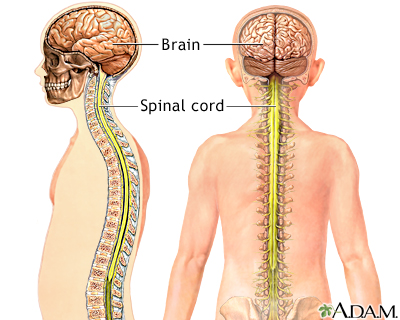
| Credits: ADAM education. |
What is the foramen magnum?
Most anatomic designations originate from Ancient Greek and Latin. Both words in foramen magnum come from Latin: foramen means "hole" and magnum "great".
The foramen magnum represents a large oval opening in the occipital bone that exists in the base of the skull. It is one of the several oval or circular openings (foramina is the plural of foramen) in the base of the skull. The spinal cord, an extension of the medulla, passes through the foramen magnum as it exits the cranial cavity through a natural opening or passage, especially one into or through a bone. Radiopaedia
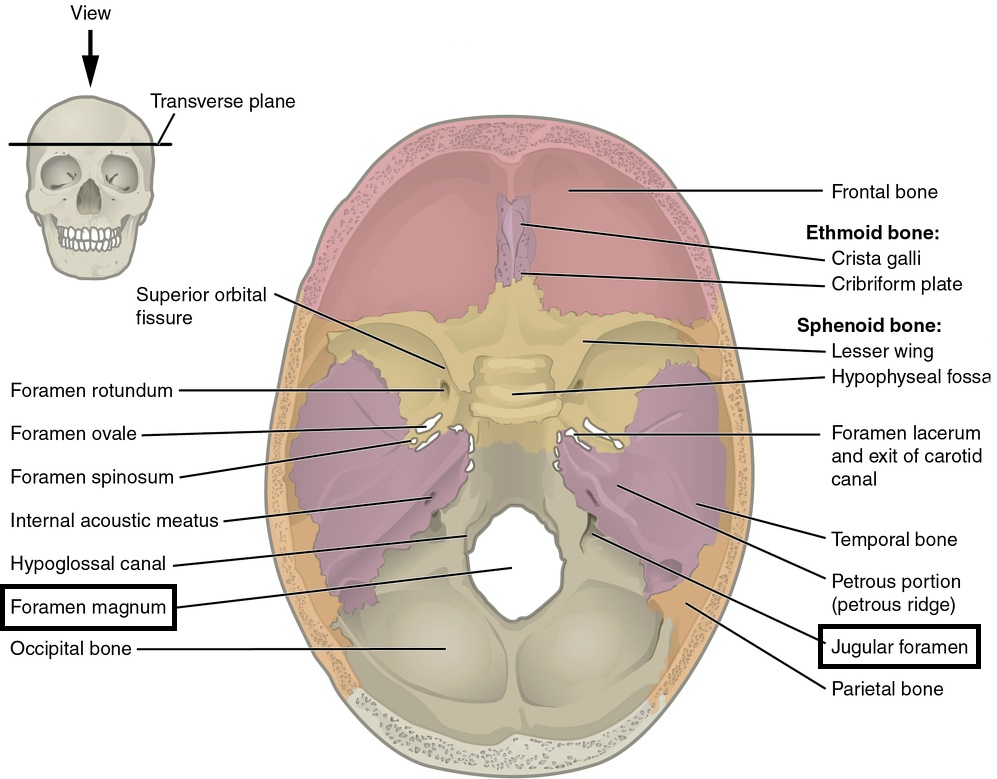
| View from inside the skull, looking from above. Case courtesy of OpenStax College, Radiopaedia.org, rID: 42751 |
|
Medulla oblongata and foramen magnum animation. The medulla oblongata, or just medulla, is a transition between the lower part of the brain (the pons) and the spinal cord. |
The foramen magnum is a fundamental component in the complex interaction of bony, ligamentous, and muscular structures composing the craniovertebral junction. Shape and size of the foramen are critical parameters for the manifestation of clinical signs and symptoms in craniocervical pathology.
Among developmental and acquired craniocervical junction disorders, achondroplasia is the most commonly reported. Tubbs R. et al., 2010
Achondroplasia results in abnormal endochondral bone formation at the cranial base resulting in a narrow cervical spinal canal, foramen magnum (Mukherjee D. et al., 2014) and jugular foramina which further leads to ventricular dilatation and prominence of the emissary veins. Some degree of ventriculomegaly (increased volume of the ventricles) is present in almost all children with achondroplasia. Bosemani et al., 2014
The presence of prominent emissary veins and meningeal veins (the veins visible in the forehead of many children with achondroplasia) supports the role of collateral vessel formation to compensate for intracranial venous hypertension and increased Cerebrospinal Fluid (CSF) pressures. Bosemani T. et al., 2014
| Credits: Bosemani et al., 2014 |

| Age controls are in this study, children of similar age without achondroplasia. Credits: Bosemani et al., 2014. |
The shape of the FM is variable and the size of the foramen magnum in patients with achondroplasia was small at all ages, particularly in those with serious neurological problems. Shepur M., et al., 2014
Babies with achondroplasia have significantly smaller foramen magnum diameters than unaffected babies, and this difference persists across the lifespan. DelRosso L., Gonzalez-Toledo E., Hoque R., A Three-Month-Old Achondroplastic Baby with both Obstructive Apneas and Central Apneas, 2013
In the next image it is possible to see the size of the foramen magnum (dark circle) in a baby with achondroplasia.


| Clinical case: a 3 months old baby with achondroplasia. Mild foramen magnum narrowing without evidence of cervicomedullary junction stenosis. Credits: DelRosso L., Gonzalez-Toledo E., Hoque R., 2013 |
What is cervicomedullary junction (CMJ) compression?
As the name implies, CMJ is the region where the brainstem (the medulla) continues as the spinal cord. A lesion located in this region affects either the brainstem or cervical cord or both depending on its extent and pathology. Involvement of brainstem is manifested as cranial nerve palsies, decreased respiratory drive, long tract signs: clonus, muscle spasticity (stiffness) or bladder involvement that usually indicate a lesion in the middle or upper parts of the spinal cord or in the brain and hydrocephalus if there is obstruction of the fourth ventricle. Nair A., et al. 2014
The most serious neurological complication in patients with achondroplasia is cervicomedullary junction (CMJ) compression caused by a tight, deformed foramen magnum. Compression at the foramen magnum can result in cervical myelopathy manifested as clonus and hyperreflexia, hypotonia, sleep apnea, and even sudden death. Due to the potentially lethal complications associated with symptomatic disease, neurosurgical decompression has been used to widen the foramen magnum and relieve the pressure on the emerging cervical cord. Fortunately, most children with achondroplasia do not suffer neurological symptoms and achieve normal motor and intellectual development without surgical intervention (Mukherjee D. et al., 2014).
Monitoring the growth of the Foramen magnum in achondroplasia
The foramen magnum size increases slowly in achondroplasia, but does increase with age. Sudden infant death has been described in achondroplastic individuals, but this usually occurs when these individuals are awake and is associated to marked hypotonia, large head size and cranial vein dilatation... Almost all children will gain significant muscle tone by age 2 or 3 years old and catch up on all motor milestones. This is probably due to the fact the foramen magnum size increases faster than cervical cord volume, thus relieving pressure on the cord. Thus the severe hypotonia on achondroplasia is self limited. Only those with significant neurological impairment and increased intraventricular pressure should require surgery. Nicoletti B., et al., Human Achondroplasia: A Multidisciplinary Approach, Volume 48 of Basic Life Sciences, Springer US, 2012
Taken from a very old paper:
The fitted nonachondroplastic foramen magnum growth curves demonstrate that the maximum growth occurs in the first 18 months and slows thereafter. Indeed, the sagittal dimension almost doubles within the first 2 years, while the transverse dimension (horizontal plane that divides the head into top and bottom parts) enlarges by half the original dimension. Growth of this area is essentially complete by 5 years of age. Hetch J., et al.,1989
Foramen magnum growth chart

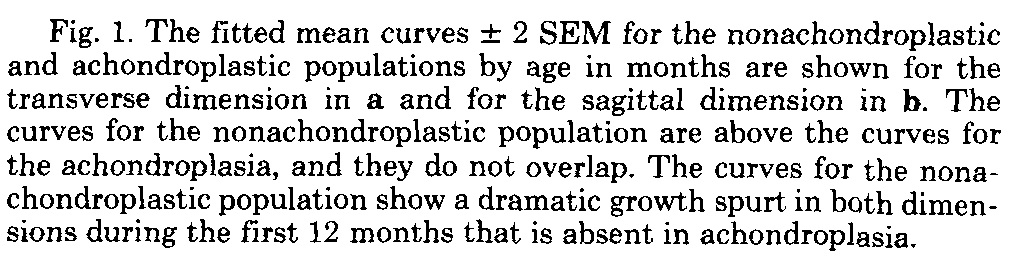
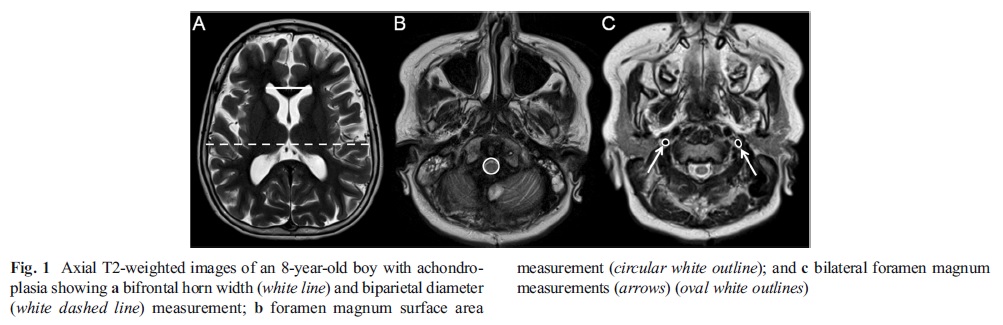
The achondroplastic foramen magnum is small at birth and the curves demonstrate that in achondroplasia, during the first year of life, the transverse dimension (fig1a) is the most severely impaired and that growth throughout life is negligible. These curves suggest that foramen magnum growth is severely impaired than can solely be attributed to abnormal endochondral growth. In the foramen magnum area, the early growth spurt (vertical line in fig 1, around 12 months of age) is absent in the transverse dimension, suggesting that other disruptive processes in achondroplasia contribute to the abnormal development of the foramen magnum. There is a premature fusion and aberrant development of the posterior synchondroses, that should normally occur by 7 years but in achondroplasia premature fusion has been observed as early as 1 year. Hetch J et al., 1989
The development of the skull base occurs mainly at the growth centers called synchondroses: intersphenoid, spheno-occipital and intraoccipital synchondroses. FGFR3 mutation accelerates ossification of cartilages in these synchondroses and causes early closure. This early closure can be the main reason of hypoplasia of the skull base in ACH. Hetch J et al., 1989
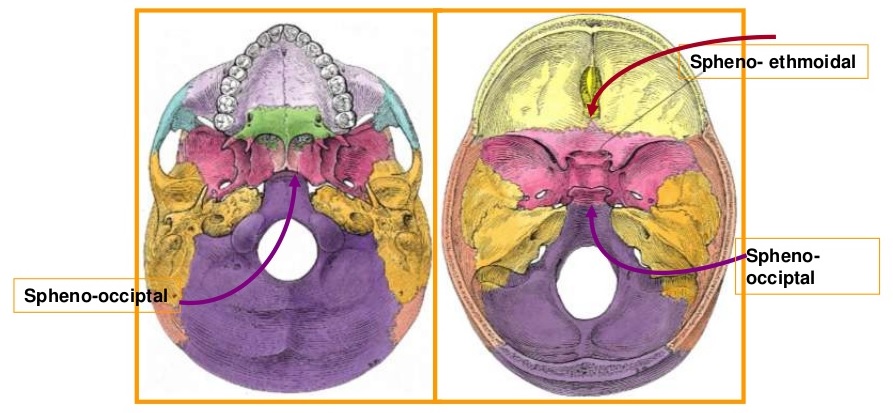
| Left: view from beneath the skull. Right: view inside the skull base. Credits: Al-Zubair N., 2013 |

| The anatomy of the skull base. There are some synchondroses of the intra- or inter-bones of the skull base. Credits: Nakai Y., et al., 2015 |
1. Despite stenosis of foramen magnum and jugular foramina, only 10-15% of children develop progressive hydrocephalus, requiring neurosurgical treatment. Bosemani T. et al., 2014
2. The absence of correlation between degree of ventriculomegaly and severity of foramen magnum or jugular foramina stenosis suggests that the decision for neurosurgical intervention cannot be taken on the basis of individual neuroimaging findings alone. Bosemani T. et al., 2014
3. It is unclear whether the absolute dimension of the foramen magnum is helpful in determining which patient will benefit from decompression. The American Academy of Pediatrics recommends an initial evaluation with a thorough neurological history, complete physical examination, neuroimaging, and polysomnography. DelRosso L. et al., 2013
4. "Only those with significant neurological impairment and increased intraventricular pressure should require surgery" Nicoletti B et al., 2012. This conclusion is very important in the evaluation of young children with achondroplasia. Medicine and mathematics are not the same science and in medicine "1 plus 1 is not equal two". This example was used to say that there are many factors involved in assessing a baby with achondroplasia as well the individual singularity, that has to be taken in account when deciding for a decompression surgery in a child with achondroplasia younger than 2 years-old. Many neurosurgeons without experience in achondroplasia cases, that face a baby with achondroplasia for the first time, with a MRI with a narrow foramen magnum, will encounter a huge challenge in evaluating the risk of cervical myelopathy and the exact need for decompression surgery.
5. Foramen magnum dimension should be regularly evaluated during early pediatric ages, and the data used to develop a better natural history guide for achondroplasia.
5. Foramen magnum dimension should be regularly evaluated during early pediatric ages, and the data used to develop a better natural history guide for achondroplasia.
6. New medicines developed for achondroplasia should act directly at the foramen magnum area and reduce the synchondrosis' early closure in achondroplasia.

